Is It Too Early for Hospice? Why Timing Matters More Than You Think
- HOME
- BLOG
July 3, 2026
- Hospice care is available to patients with a terminal illness and a physician-estimated prognosis of six months or less, but many families wait too long to explore it.
- Choosing hospice does not mean giving up. It means shifting the focus of care toward comfort, dignity, and quality of life.
- Patients who start hospice earlier often experience better symptom management, fewer unnecessary hospitalizations, and more meaningful time with family.
- Medicare, Medi-Cal, and most private insurance plans cover hospice services at no out-of-pocket cost to the patient.
- You can leave hospice at any time if your condition improves or you choose to resume curative treatment.
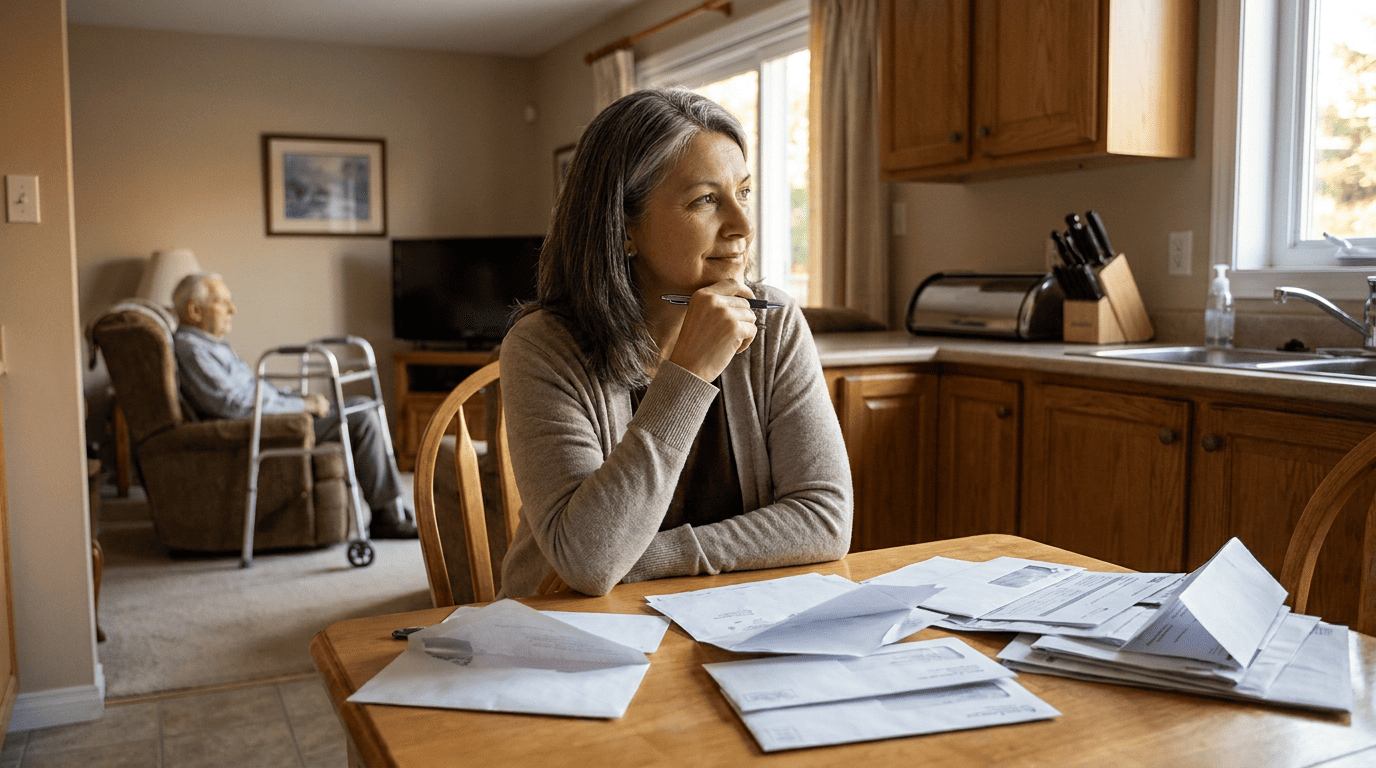
The Hardest Conversation Nobody Prepares For
A doctor says the word “hospice,” and the room goes quiet. Most families hear it as a verdict. A line being drawn. Something final.
That reaction is completely understandable. For many people, hospice is connected to loss, to the last few days, to the idea that medicine has nothing left to offer.
But here is what catches most families off guard: hospice was never designed to be a last resort. It was built to provide months of structured medical support, emotional care, and practical help for patients and their families during a difficult chapter of life. The problem is that most people only learn that after the fact.
According to the National Hospice and Palliative Care Organization (NHPCO), the median length of stay in hospice in the United States is approximately 17 days — a fraction of the time hospice is designed to serve. Many clinicians, families, and patients say the same thing afterward: we should have started sooner.
This article explains what hospice actually provides, how to recognize when it may be appropriate, and why exploring it earlier can lead to better outcomes for patients and families alike.
What Hospice Care Actually Means

Hospice is a specialized form of medical care for people living with a terminal illness when curative treatments are no longer effective or no longer align with the patient’s goals. Rather than attempting to cure the underlying disease, hospice focuses on managing symptoms, controlling pain, and supporting the patient’s emotional and spiritual well-being.
Under Medicare guidelines, a patient qualifies for hospice when two physicians certify a terminal prognosis of six months or less if the illness follows its expected course. But that six-month estimate is a clinical guideline, not an expiration date. Patients who stabilize or improve can be recertified, and those who no longer meet hospice criteria can return to curative care at any time.
What a Hospice Team Typically Includes
- Physicians who specialize in pain and symptom management
- Registered nurses who coordinate day-to-day clinical care
- Certified home health aides for personal care and bathing assistance
- Medical social workers who help with advance directives, insurance questions, and family dynamics
- Chaplains and spiritual counselors
- Bereavement counselors who support families for up to 13 months after a patient's passing
- Trained volunteers who provide companionship, respite support, and practical help
This team works together under what Medicare calls the interdisciplinary group (IDG) model. The patient’s own physician can remain involved in directing care, with the hospice medical director providing additional oversight.
Why Most Families Wait Too Long to Consider Hospice
Delay is the norm, not the exception. Several factors contribute to late hospice referrals, and almost none of them have to do with a lack of caring.
Misunderstanding What Hospice Provides. Many families associate hospice exclusively with the final hours or days of life. The reality is far broader — hospice delivers ongoing, structured medical care that can last weeks or months, including regular nurse visits, medication management, coordination with specialists, equipment delivery, and 24/7 access to a clinical team by phone.
Confusing Hospice With Giving Up. Choosing comfort-focused care is not the same as choosing to stop caring. It is a deliberate shift in priorities: from fighting a disease that cannot be reversed to making sure the patient lives each day with as little suffering and as much meaning as possible.
Waiting for a Doctor to Bring It Up. Physicians often delay hospice conversations because they are uncertain about prognosis, worry about removing hope, or feel the patient is not ready. As a result, families sometimes don’t learn about hospice until a crisis forces the issue.
Cultural and Personal Beliefs. In many cultures, discussing death openly is discouraged. Families may view hospice as a cultural taboo or interpret the recommendation as an insult to the patient’s strength. These beliefs are deeply personal, and hospice teams understand and respect them. But when those beliefs delay access to symptom management and caregiver support, patients and families carry a burden they don’t have to carry alone.
Signs That Hospice May Be Worth Exploring
- Repeated hospitalizations or emergency room visits within the past six months
- A significant decline in the patient's ability to perform daily tasks such as bathing, dressing, eating, or walking
- Unintentional weight loss of 10% or more over six months
- Increasing difficulty managing pain, nausea, shortness of breath, or other symptoms despite treatment
- The patient or family has asked, "Would you be surprised if this person died within the next year?" and the honest answer is no
- Treatments are being continued primarily to feel like "something is being done" rather than because they are improving quality of life
- Trained volunteers who provide companionship, respite support, and practical help
- The primary caregiver is physically or emotionally exhausted
- Family members are making complex medical decisions without adequate clinical support
- The caregiver's own health is declining
- The family disagrees about next steps and has no neutral clinical team to guide the conversation
What Changes When Hospice Starts Earlier
Families who engage hospice services weeks or months before the end of life consistently describe a different experience than those who come to hospice in a crisis.
Better Pain and Symptom Control. When a hospice team has time to assess the patient’s needs, adjust medications, and establish a care routine, symptom management tends to be more effective.
Fewer Unnecessary Hospital Visits. Hospice teams provide 24/7 clinical phone support and can deploy nurses for urgent home visits, reducing the likelihood of 911 calls or ER visits during a symptom flare.
More Time for Meaningful Conversations. When a family is not consumed by logistics and crisis management, they can focus on what actually matters: being present with the person they love.
Stronger Caregiver Support. Social workers, chaplains, and bereavement counselors support the entire family. Home health aides provide hands-on personal care that gives primary caregivers a chance to rest. Respite care allows the caregiver to step away for a few days while the patient is cared for in a supervised setting.
Early vs. Late Hospice Enrollment: What Families Experience
Factor | Earlier Enrollment | Late Enrollment (< 7 days) |
Symptom management | Proactive, gradual adjustments | Reactive, crisis-driven |
Caregiver burden | Shared with hospice team | Falls largely on the family |
Hospitalizations | Significantly reduced | Often continues until enrollment |
Family conversations | Time to talk openly | Rushed, emotional decisions |
Bereavement support | Relationship with team established | Limited connection with counselors |
Patient comfort | Well-managed over time | May not be fully achieved |
Four Levels of Hospice Care Under Medicare
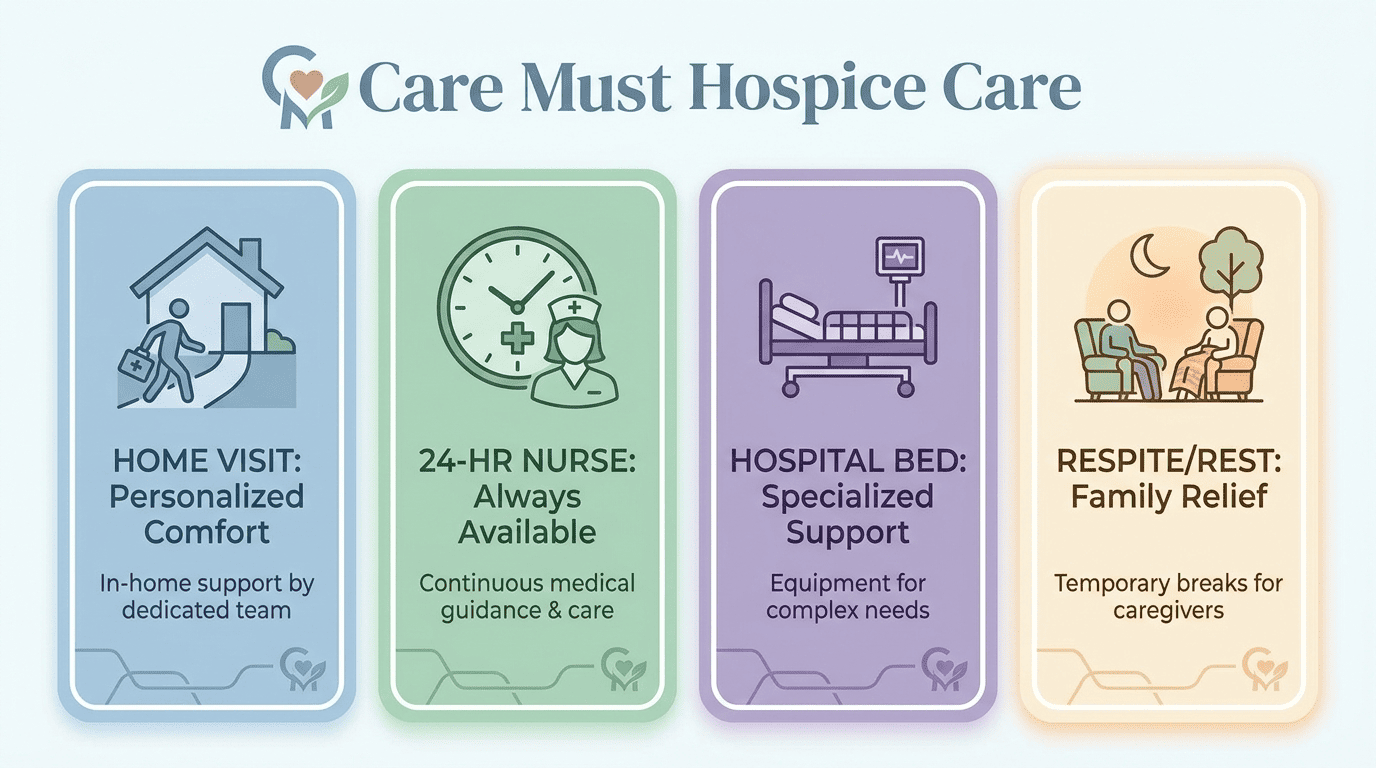
- Routine Home Care — the most common level. The patient receives care at home (or wherever they live, including assisted living or a nursing home) with scheduled visits from nurses, aides, social workers, and chaplains.
- Continuous Home Care — when a patient experiences an acute symptom crisis, hospice can provide nursing care at home for up to 24 hours a day until symptoms are controlled.
- Inpatient Care — if symptoms cannot be managed at home, the patient may be temporarily transferred to a facility for intensive symptom management.
- Respite Care — short-term inpatient care (up to five consecutive days) to give the primary caregiver a break. Medicare covers the cost with a small copayment.
Hospice Focuses on Living, Not Dying
This is the part that surprises most people. Hospice care is not about waiting for death. It is about making sure that the days a patient has left are spent with as much comfort, connection, and personal meaning as possible.
Birthdays still get celebrated. Grandchildren still climb onto the bed. A favorite meal still brings comfort on a hard day. These moments do not stop because someone is on hospice. In many cases, hospice is what makes them possible, because pain is managed, symptoms are controlled, and the family is not drowning in logistical decisions.
At Care Must, this philosophy is reflected in everything we do. Our tagline, “Moments that matter,” describes the reason our clinical team shows up every day: to protect and create the conditions for those moments.
How Hope Changes During Serious Illness
Families often fear that hospice means losing hope. In practice, hope simply changes form.
Early in a diagnosis, hope might look like full remission. As the disease progresses, hope might shift toward better symptom control, one more holiday at home, a night without pain, or having enough energy to sit at the dinner table with family. These are not lesser forms of hope — they are specific, realistic, and deeply meaningful. Hospice recognizes that and builds care plans around what matters most to the individual patient.
How Hospice Is Paid For
- Medicare Part A covers hospice care with no out-of-pocket costs for services related to the terminal illness, including medications, equipment, and supplies.
- Medi-Cal (California Medicaid) also covers hospice services.
- Most private insurers and HMOs include hospice as a covered benefit.
- Veterans may be eligible for hospice through the VA healthcare system.
Patients are responsible for a small copayment (up to $5) for outpatient prescriptions related to symptom management. For respite care, the copayment is 5% of the Medicare-approved amount. Beyond that, hospice services are fully covered.
You Can Leave Hospice at Any Time
A decision that worries many families is the fear that choosing hospice is irreversible. It is not.
Patients can revoke their hospice election at any time and return to standard Medicare coverage and curative treatment. If a patient’s condition improves and they no longer meet hospice criteria, they are discharged from the benefit and can re-enroll later if their condition changes again. This flexibility is built into the Medicare hospice benefit by design, so families are never locked into a decision they are no longer comfortable with.
How to Start the Hospice Conversation With Your Family
Bringing up hospice is difficult. There is no script that makes it easy. But there are approaches that tend to work better than others.
- Start with questions, not statements. Ask your loved one what matters most to them right now. Ask what they are afraid of. Ask what a good day looks like.
- Separate learning from deciding. Requesting information about hospice does not mean you are enrolling. A consultation is just a conversation.
- Include the patient’s physician. A physician who knows the patient’s medical history can help the family understand the prognosis and what hospice would look like in their specific situation.
- Talk to a hospice provider directly. Most hospice organizations, including Care Must, offer free consultations with no obligation. A clinical team member can visit the home, assess the patient’s needs, and walk the family through exactly what services are available.
- Give everyone time to process. These conversations rarely happen in one sitting. Be patient with family members who need more time, and be honest about your own feelings.
How Care Must Supports Families in San Jose and Beyond
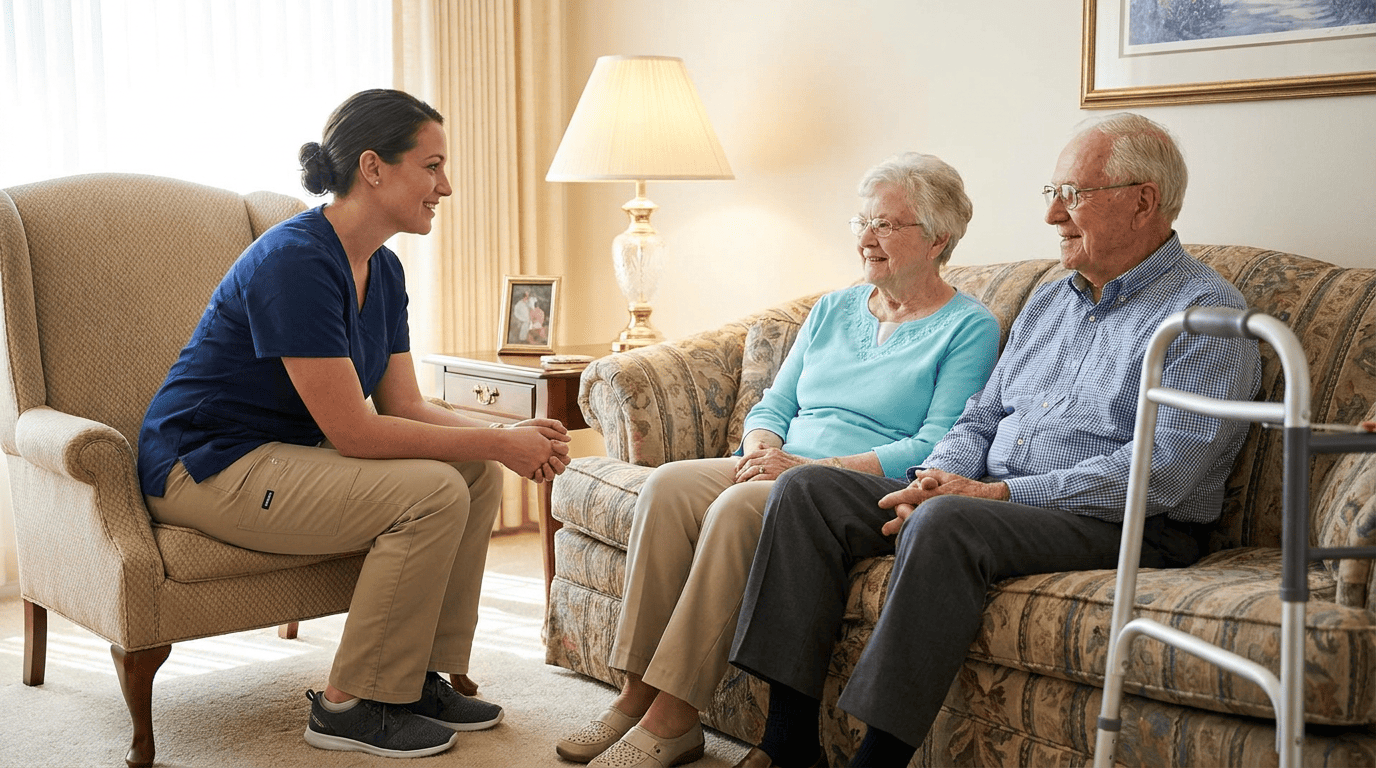
Care Must is a licensed home health and hospice provider based in San Jose, California, offering a full range of hospice services including routine home care, continuous nursing care, inpatient care, and respite care. Our interdisciplinary team includes physicians, registered nurses, certified home health aides, social workers, chaplains, and bereavement counselors.
We also provide palliative care, transitional care, and grief support services designed to meet the needs of patients and families at every stage of a serious illness. Our clinical team is available 24 hours a day, seven days a week, and we work closely with each patient’s primary physician to ensure continuity of care.
If you are wondering whether it is the right time to explore hospice for someone you love, we encourage you to call us at (408) 755-1215 or visit our Request a Consultation page. There is no pressure and no obligation.
The Question Worth Asking
Is it too early for hospice? Maybe. Every situation is different.
But asking the question is never too early. Learning about your options does not commit you to anything. It puts you in a stronger position to make decisions that reflect your loved one’s wishes, your family’s values, and the kind of care that leads to less suffering and more meaningful time together.
If more support is available today, there is no reason to wait until a crisis to find out.
Frequently Asked Questions
No. Hospice shifts the focus of care from trying to cure a disease to managing symptoms, controlling pain, and improving quality of life. It is an active form of medical care delivered by a specialized team. Patients who choose hospice are choosing comfort and dignity.
A patient may be eligible for hospice when a physician estimates a life expectancy of six months or less if the illness follows its expected course. However, many patients benefit from hospice services for weeks or months. Earlier enrollment typically leads to better symptom control, more caregiver support, and a calmer experience for the entire family. See our eligibility guidelines for details.
Yes. Patients can revoke their hospice election at any time and return to standard Medicare coverage and curative treatment. If a patient's condition improves beyond hospice eligibility, they are discharged and can re-enroll later if needed.
Medicare Part A, Medi-Cal, and most private insurance plans cover hospice care. Under Medicare, there is no cost for hospice services related to the terminal diagnosis, including medications, equipment, and medical supplies. A small copay may apply for prescriptions and respite care.
Hospice care is most commonly provided at home, but it can also be delivered in assisted living facilities, nursing homes, or inpatient hospice units when needed. Care Must's Routine Home Care model brings the hospice team to wherever the patient lives.
A hospice interdisciplinary team includes physicians, registered nurses, home health aides, medical social workers, chaplains, bereavement counselors, and trained volunteers, all coordinating under Medicare's IDG model.
Hospice bereavement counseling is available to families for up to 13 months after a patient's passing, including individual counseling, support groups, and referrals to community resources. Learn more about grief and bereavement services.
Routine Home Care, Continuous Home Care, Inpatient Care, and Respite Care — each designed for a different level of clinical need, all covered under Medicare Part A.
Hospice is available for any terminal illness, including but not limited to cancer, heart failure, COPD, Alzheimer's disease, stroke, kidney disease, liver disease, ALS, and HIV/AIDS. Eligibility is based on the patient's overall clinical trajectory, not a specific diagnosis.
You can call Care Must at (408) 755-1215 or visit our Request a Consultation page to schedule a free, no-obligation consultation. A member of our clinical team will meet with the patient and family to assess needs and explain available services.

